”
”
“We are over – treating a large number of healthy women who have a relatively minor risk of fracture while we are ignoring a sizable number of individuals at high risk of fracture”-Dr. Robert Neer (Los Angeles Times, June 13, 2005)
Osteoporosis authorities have long known this, but the public is still misled into thinking that ‘osteopenia” is a disease. In 2005 osteoporosis authority Dr. Stephen Cummings explained to the Los Angeles Times that osteopenia has “no medical meaning” and as he went on to say, “I’ve seeing patients who come in scared they will become disabled soon because they have this “disease called osteopenia, when in fact they are normal for their age”. Dr. Robert Neer, then director of the Osteoporosis Center at Massachusetts General Hospital goes on further to explain.
Currently 44 millions person over 50 in the U.S. have a bone density that classifies them as having ”osteopenia”
Being told that you have “osteopenia” by itself tells us very little about the strength of the bone. Whether the designation of osteopenia carries any significance or not will depend on individual’s total load of fracture risk factors. My fracture risk assessment will help you understand your personal total load of many common bone weakening factors.
The “osteopenia” range is very wide and translates into bone mass that is anywhere from 10 to 30% below the average young person. So just as a person might have a weight that is 10% or even 30% less than the average young person so might have a bone density that is that much lower than the average young person.
Originally there was little use for the term “osteopenia” and osteoporosis was defined only after the fact by a low trauma fracture. Beginning in the late 1980’s, however, the widespread use of bone density testing eventually allowed for the establishment of the ”average” bone density. Armed with bone density testing data, a handful of male scientists met in 1994 and redefined both ‘osteoporosis” and “osteopenia” in terms to bone density.
“Osteoporosis”was defined as a bone density that was -2.5 standard deviations or more below that of the average young person. “Osteopenia” was the descriptor for those who had a bone density anywhere between-1 and -2.49 standard deviations of the average young person of the same sex.


As it turns out the bone density testing used today is greatly influenced by bone size, in fact scientists call this a measurement in “aerial” bone density and not a strict measurement of bone density itself. Those people with smaller bones come up with lower readings on the bone density test. For more information on this, see my blog.
This direct linear relationship between body weight and bone density is clearly illustrated in the graph below, which plots bone density against body weight in a sample of over 22,000 women and men in the U.S.
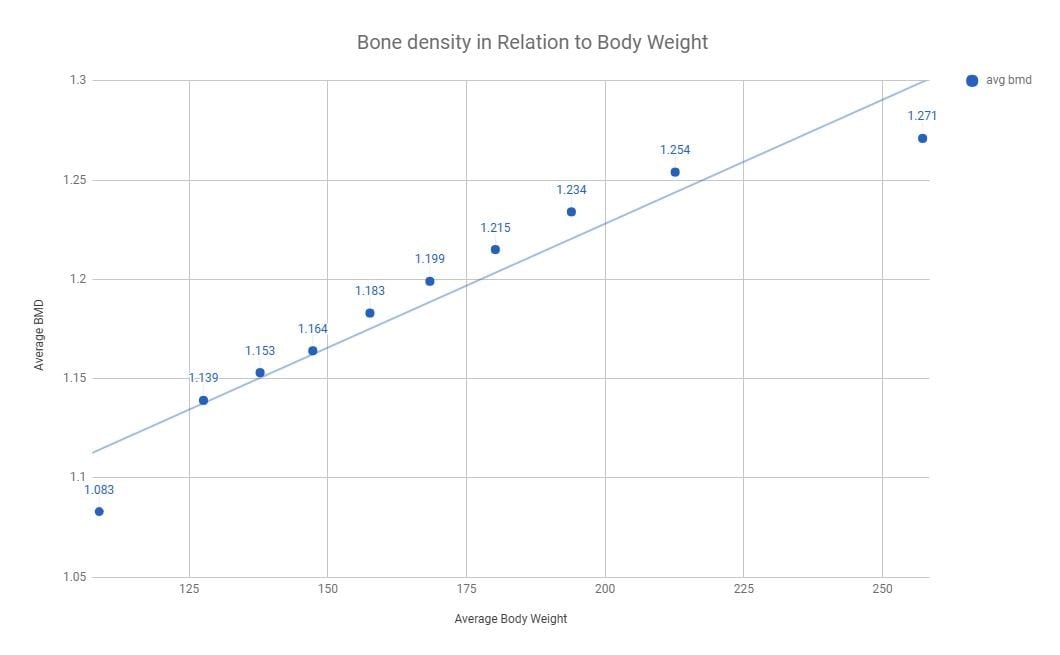
Personal communication with Dr. Gilbert Kaats, Integrative Health Technologies, San Antonio, TX

44 million people in the US have “osteopenia” and many of them are healthy, small-boned, lighter weight people.
We will be writing more about the different types of osteopenia to help you distinguish when having osteopenia might be a real sign of increased fracture risk. For now, here is a simple checklist of when osteopenia likely suggests increased fracture risk:
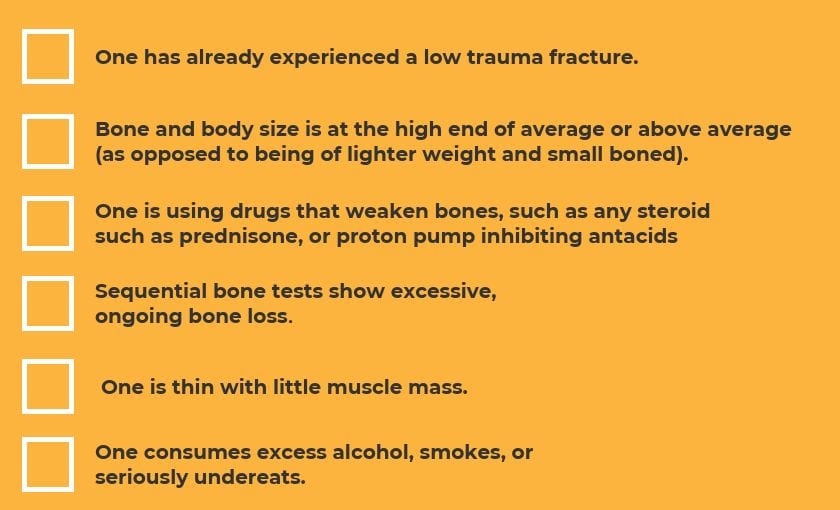

Researchers note that low bone mass accounts for less than 1/2 of all low trauma “osteoporotic” fractures. Actually, there are many other fracture risk factors more important than bone density.For example, a history of fracture after 40, or having a parent fracture a hip are stronger predictors of fracture than bone mineral density and these factors are independent of bone density. Also several studies show that you can have similar bone densities with different fractures rates. For example, the same bone mass in northern Europe is associated with a substantially higher fracture risk than that in southern Europe. Further, at the same bone density, advancing age by itself increases fracture risk.
I have written numerous times on why bone density is not a good indicator of fracture risk. Take a look at this recent blog where I outline the concerns of the FRAX calculations.

Because “osteopenia” is defined by a statistical calculation, some 15% of any population will fall into this statistical category. Many of these are healthy individuals with a low risk of fracture. Fractures result from multiple risk factors, as detailed below…Who Will Fracture
In fact there are 3 very important things you should remember when you’re told you you have an osteopenia diagnosis.

Your fracture risk is determined by having multiple risk factors, of which there are over 125 in fact.
For example, as early as 1995, Dr. Cummings and colleagues reported that hip fracture risk was 17 times greater among the 15% of women who had five or more risk factors (without accounting for bone density) than the 47% of women with 2 or 3 risk factors.
These factors can include but are not limited to:
- medication use
- smoking
- excessive alcohol use
- premature ovarian failure
- kidney impairment
- gastrointestinal conditions
- endocrine conditions
- nutritional factors (including a high-acid diet)
- lifestyle factors (lack of exercise or too much worry).
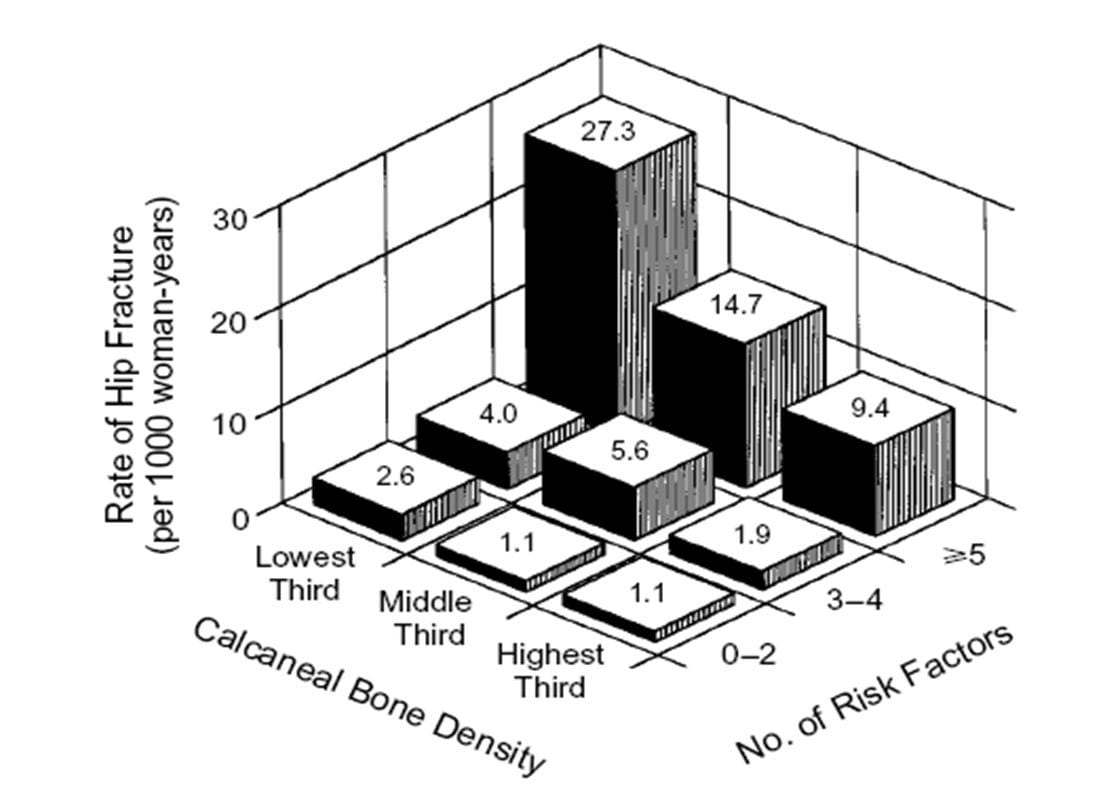
Annual Risk of Hip Fracture According to the Number of Risk Factors and the Age-Specific Calcaneal Bone density
Cummings, S.R., et al. N Engl J Med. 1995, 332:767-773

Here’s another way to look at potential secondary causes of bone weakness.
8. In most cases bone drugs are largely ineffective and unnecessary for osteopenia. There’s growing, thoughtful medical consensus that bone drugs are largely ineffective and unnecessary for preventing fractures in those with osteopenia, and universal recommendations for preventing osteopenic fractures focus on lifestyle factors instead of drugs.
Read More…